
SAS Program
Research Question: Is lower income associated with worse health from a global perspective?
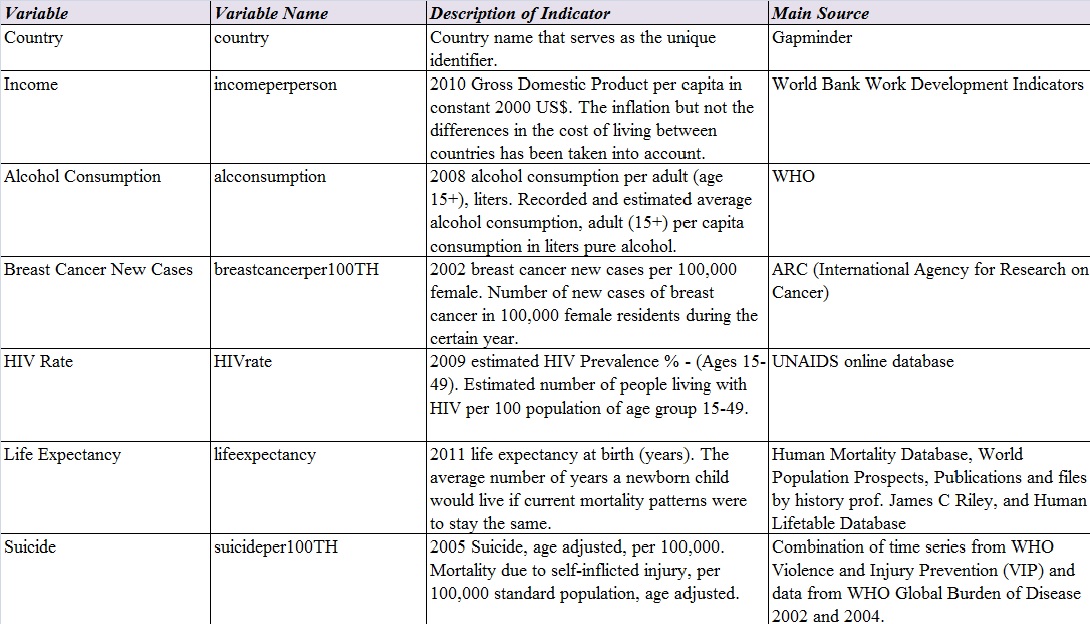
Please click here for my codebook.
Please click here for the entire SAS program. (Please click the following images for larger images)
1. Assign label names for variables

2. Set unknown values to missing values and create a secondary variable called HIVper100TH

3. Group values of the variables


4. Set range of values (completed in week 2) and interpreted responses (completed in week 3) for variables






5. Run frequency distributions tables that show groups of values

OUTPUT (FREQUENCY TABLES)
Please click here for all frequency tables.

Income per person by country was divided into 5 groups. 20% of countries had the lowest income per person of US$559 or less. The second group (21%-40% of countries) had income between US$560 and US$1,845. The third group (41%-60%) had income between US$ 1,846 and US$4,700. The fourth group (61%-80%) had income between US$4,701 and US$13,578. The 20% with highest income had income between US$13,579 and US$105,148. The range of income was larger for groups with higher income. There were no data for 23 countries, and those were marked as missing data.

The estimated average alcohol consumption per capita in liters were divided into 5 groups, 5 liters in each group. There were 43.32% of countries with alcohol consumption between 0 and 5 liters. There were 32.62% and 18.18% with alcohol consumption between 5.01 and 10 liters and between 10.01 and 15 liters respectively. There were only 5.88% with alcohol consumption between 15.01 and 25 liters. There were no data for 26 countries, and those were marked as missing data.

The numbers of breast cancer new cases in 100,000 females were divided into 5 groups. There were 28.9% of countries had 0 to 22 new cases. There were 39.31% and 17.92% had numbers of new cases between 22.1 and 44 and between 44.1 and 66 respectively. There were less countries with larger numbers of new cases; 9.83% and 4.05% had numbers of new cases between 66.1 and 88 and between 88.1 and 110 respectively. There were no data for 40 countries, and those were marked as missing data.

The estimated numbers of people living with HIV by country were divided into 5 groups. Secondary variable (HIV number per 100,000 people) was created from the primary variable (HIV rate/number in 100 people) because the numbers of breast cancer new case and suicide were presented with numbers “in 100,000 people”. 30% of countries had the lowest numbers of people living with HIV, between 0 and 100 people in 100,000 people. The second group (31%-40%) had the numbers of people living with HIV between 101 and 200. The third group (41%-60%) had numbers between 201 and 600. The fourth group (61%-80%) had numbers between 601 and 1,800. 20% with the highest numbers of people with HIV were between 1,801 and 25,900. The groups with larger numbers of people with HIV had larger range than the groups with smaller numbers of people with HIV. There were no data for 66 countries, and those were marked as missing data.

The average numbers of years a newborn child would live were divided into 5 groups, 10 years in each group. There were 4.71% of countries with life expectancy between 40.001 and 50 years of age. There were 15.18% and 19.9% with life expectancy between 50.001 and 60 years old and between 60.001 and 70 years old respectively. The highest percent of life expectancy (48.17%) were in the group between 70.001 and 80 years of age. There were 12.04% with life expectancy between 80.001 and 90 years of age. There were no data for 22 countries, and those were marked as missing data.

The numbers of suicide in 100,000 people were divided into 5 groups, 8 suicide cases in each group. There were 46.07% (highest percent) of countries with suicide numbers between 0 and 8. There were also 42.41% with suicide numbers between 8.001 and 16. The numbers of countries were decreased when the numbers of suicide increased. There were 11.52% with suicide numbers between 16.001 and 40. There were no data for 22 countries, and those were marked as missing data.














You must be logged in to post a comment.